Why Brain Cancer Is So Dangerous: A Neurologist's Perspective
Brain cancer is uniquely lethal — not because tumors are always large, but because of where they grow, how they spread, and what they disrupt. Here is what makes it so dangerous.
Few diagnoses carry the weight of a brain tumor. Even when a growth is technically small, its location alone can change how a person speaks, moves, remembers, or feels. That is the cruel arithmetic of brain cancer: millimeters matter in a way they do not in most other organs.
As clinicians, we are often asked the same question by patients and families: why is this one so hard to treat? The honest answer is that brain cancer combines several biological and anatomical disadvantages that rarely line up in other tumors. Understanding those reasons is not just academic — it shapes screening, symptoms to watch for, and the realistic expectations of treatment.
What "Brain Cancer" Actually Means
Brain cancer is an umbrella term for malignant tumors that originate in the brain (primary brain tumors) or spread to it from elsewhere (metastatic or secondary brain tumors). The most common aggressive primary type in adults is glioblastoma (GBM), a grade 4 glioma. According to the National Cancer Institute, GBM accounts for roughly half of all malignant primary brain tumors in adults, and median survival remains 12–15 months even with aggressive treatment.
Metastatic brain tumors are actually far more common than primary ones. Cancers of the lung, breast, kidney, colon, and melanoma frequently travel to the brain. When they do, the prognosis usually worsens sharply — which is itself a clue to why this organ is such a difficult battlefield.
1. The Skull Has No Room to Negotiate
Every other organ in the body has some give. The liver can swell. The intestines can shift. The lungs can compress and re-expand. The brain cannot. It sits inside a rigid bony vault with a fixed volume of about 1,400 millilitres.
When a tumor grows — or when the tissue around it swells from inflammation — pressure inside the skull rises. This is called increased intracranial pressure, and it produces the classic warning signs:
- New, persistent headaches, often worse in the morning
- Nausea or vomiting unrelated to meals
- Blurred or double vision
- Drowsiness, confusion, or personality change
- Seizures in someone with no prior history
These symptoms can appear long before a tumor is biologically "advanced." A 2 cm mass in the liver may go unnoticed for years. A 2 cm mass pressing on the brainstem can be life-threatening within weeks. This is the first reason brain cancer is so dangerous: the container is unforgiving.
2. Location Decides the Damage
A tumor in the kidney removes kidney tissue. A tumor in the brain removes who you are in pieces.
Depending on where it grows, the same biological tumor can cause:
- Frontal lobe: loss of judgment, motivation, personality changes
- Temporal lobe: memory loss, language difficulty, seizures
- Parietal lobe: trouble with spatial awareness, reading, calculation
- Cerebellum or brainstem: balance loss, swallowing problems, breathing instability
- Motor cortex: weakness or paralysis on one side of the body
This is why two patients with the same tumor type can have dramatically different experiences. It also limits how aggressively surgeons can cut. In the liver, a margin of healthy tissue can be sacrificed. In the brain, removing even a few extra millimetres near speech or motor areas can permanently disable a person. Surgeons must constantly weigh tumor control against neurological survival — a trade-off that does not exist in most other cancers.
3. The Blood–Brain Barrier Blocks Most Drugs
The brain is protected by a tightly sealed layer of cells lining its blood vessels, known as the blood–brain barrier (BBB). Its job is to keep toxins, pathogens, and large molecules out of neural tissue. Evolutionarily, that is a gift. Therapeutically, it is a wall.
Most chemotherapy drugs that work beautifully against breast or colon cancer simply cannot cross the BBB in meaningful concentrations. Even many modern targeted therapies and antibodies — the same drugs revolutionizing treatment elsewhere — struggle to get in. The few agents that do cross, like temozolomide, are limited and often lose effectiveness as tumors evolve resistance.
Researchers are now using focused ultrasound, nanoparticles, and convection-enhanced delivery to bypass the BBB, but routine clinical use is still limited. Until that changes, drug delivery remains one of the biggest reasons brain cancer outcomes lag behind cancers like thyroid or testicular cancer, where survival rates exceed 90%.
4. Glioblastoma Is Diffuse, Not a Discrete Lump
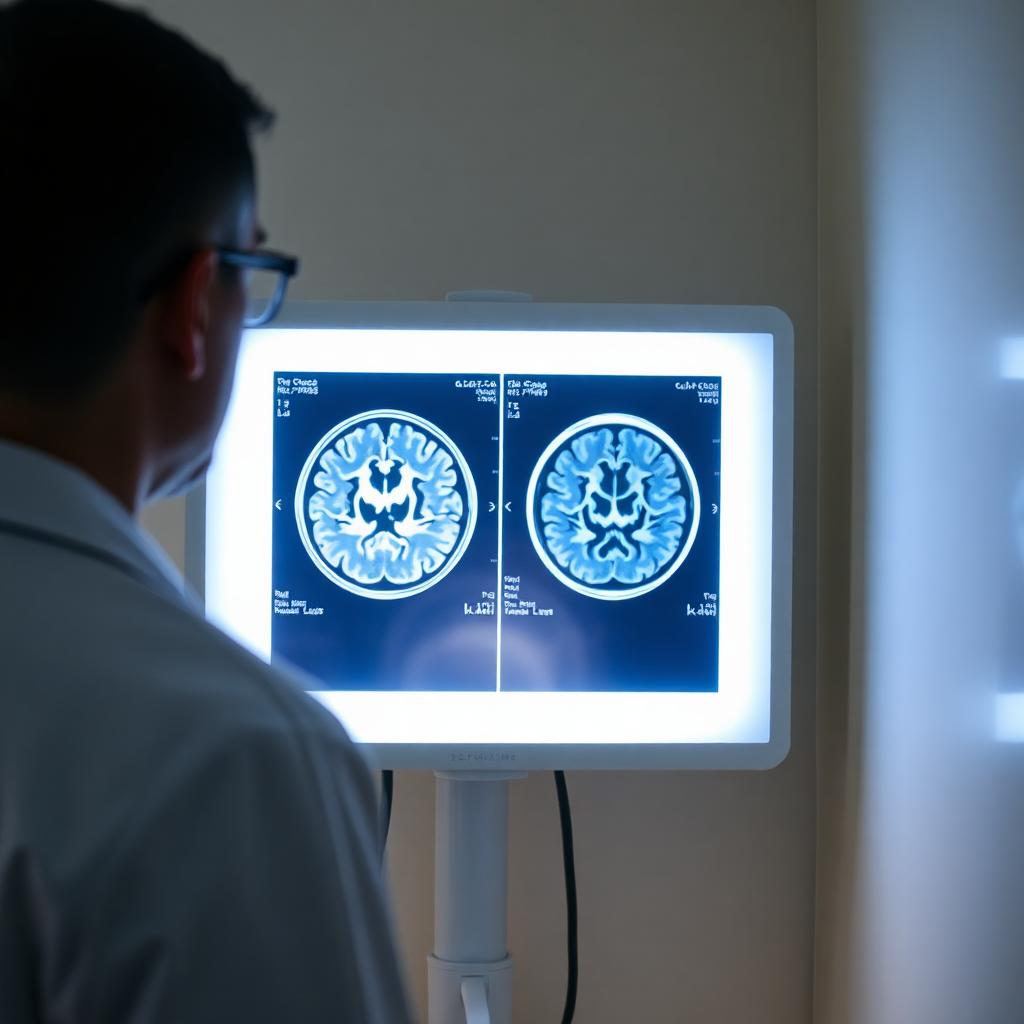
When you look at a glioblastoma on MRI, it appears as a defined mass with bright edges. The reality under the microscope is very different. Glioma cells infiltrate normal brain tissue millimetre by millimetre, threading themselves between healthy neurons. By the time surgery is performed, microscopic tumor cells already exist centimetres beyond the visible edge.
This is why "complete resection" of a glioblastoma is almost impossible. You can remove what you see and still leave behind disease that will regrow. Radiation and chemotherapy are designed to mop up those invisible cells, but resistance develops quickly. It is the biological equivalent of pulling weeds whose roots run under the entire lawn.
5. The Tumor Hides From the Immune System
Immunotherapy has transformed cancers like melanoma and certain lung cancers. The brain has been stubbornly resistant. For decades it was considered "immune-privileged," meaning immune cells were thought to barely access it. We now know they do — but glioblastoma actively builds a deeply immunosuppressive environment around itself, suppressing the very T cells that should attack it.
Clinical trials of checkpoint inhibitors, vaccines, and CAR-T therapy are ongoing and showing flickers of promise, but no immunotherapy has yet produced the dramatic responses in brain cancer that we see in other malignancies.
6. Recurrence Is Almost Universal
For most aggressive brain tumors, the question is not if they will recur but when. Glioblastomas typically recur within 6–9 months of initial treatment, often near the original surgical cavity. Second-line treatments exist, but their benefit is measured in months, not years.
This pattern is part of what makes brain cancer emotionally devastating. Patients and families adapt to the diagnosis, complete a brutal treatment course, regain some normalcy — and then face the same enemy again.
Risk Factors and Prevention: What We Actually Know
Unlike lung or skin cancer, brain cancer has few clearly modifiable risk factors. The strongest established ones are:
- Prior therapeutic radiation to the head
- Certain inherited syndromes (Li–Fraumeni, neurofibromatosis, Lynch)
- Immunosuppression, which raises the risk of CNS lymphoma
Despite popular fears, large studies have not shown a clear link between routine mobile phone use and brain cancer. The WHO's IARC currently classifies radiofrequency fields as "possibly carcinogenic" (Group 2B) — the same category as pickled vegetables — meaning the evidence is limited, not strong.
The most realistic prevention strategy is the same broad foundation that protects against many cancers: don't smoke, maintain healthy weight, manage blood pressure, and address sleep and stress. If you want a practical starting point, our guide to the 6 most important things you can do for your health covers the evidence-based habits with the largest downstream impact.
When to See a Doctor
Most headaches are not tumors. Most memory lapses are not tumors. But certain patterns deserve urgent evaluation:
- A new headache pattern that wakes you from sleep or worsens with coughing/straining
- A first-ever seizure in adulthood
- Progressive weakness, numbness, or speech change over days to weeks
- Personality or memory change noticed by family more than by the patient
- Persistent vomiting without GI cause
An MRI is the imaging test of choice, and early evaluation matters — particularly because the symptoms of brain tumors overlap with stroke, which is itself a time-critical emergency.
The Honest Outlook
Brain cancer is dangerous because nearly every weapon medicine usually relies on — drug delivery, complete surgical removal, immune attack, healing space — is blunted inside the skull. That said, the picture is not static. Survival for some pediatric brain tumors has improved dramatically. Molecularly targeted therapies for IDH-mutant gliomas are reaching the clinic. Vaccine and viral therapies are in late-stage trials. Progress is slow, but real.
For anyone living with a diagnosis — or supporting someone who is — knowledge is genuinely protective. Understanding why this disease behaves the way it does helps families ask sharper questions, choose centres of excellence, and make treatment decisions with clearer eyes.
For more evidence-based health writing, explore our full Health category or read about what vitamin D really does in the body.
FAQ
Is brain cancer always fatal?
No. Many brain tumors are benign or low-grade and can be cured or controlled for decades. Aggressive types like glioblastoma have much poorer outcomes, but survival varies enormously by tumor subtype, age, genetics, and treatment access.
Can brain cancer be detected early?
There is no routine screening test for brain cancer in people without symptoms, because the disease is relatively uncommon and MRI screening would produce too many false positives. Early detection depends on recognizing the warning signs above and seeking prompt evaluation.
Do cell phones cause brain cancer?
The best available evidence does not show a clear causal link between normal mobile phone use and brain cancer. Heavy users may want to use speakerphone or wired headsets as a precaution, but this is not a leading risk factor.


